Not a Mockup
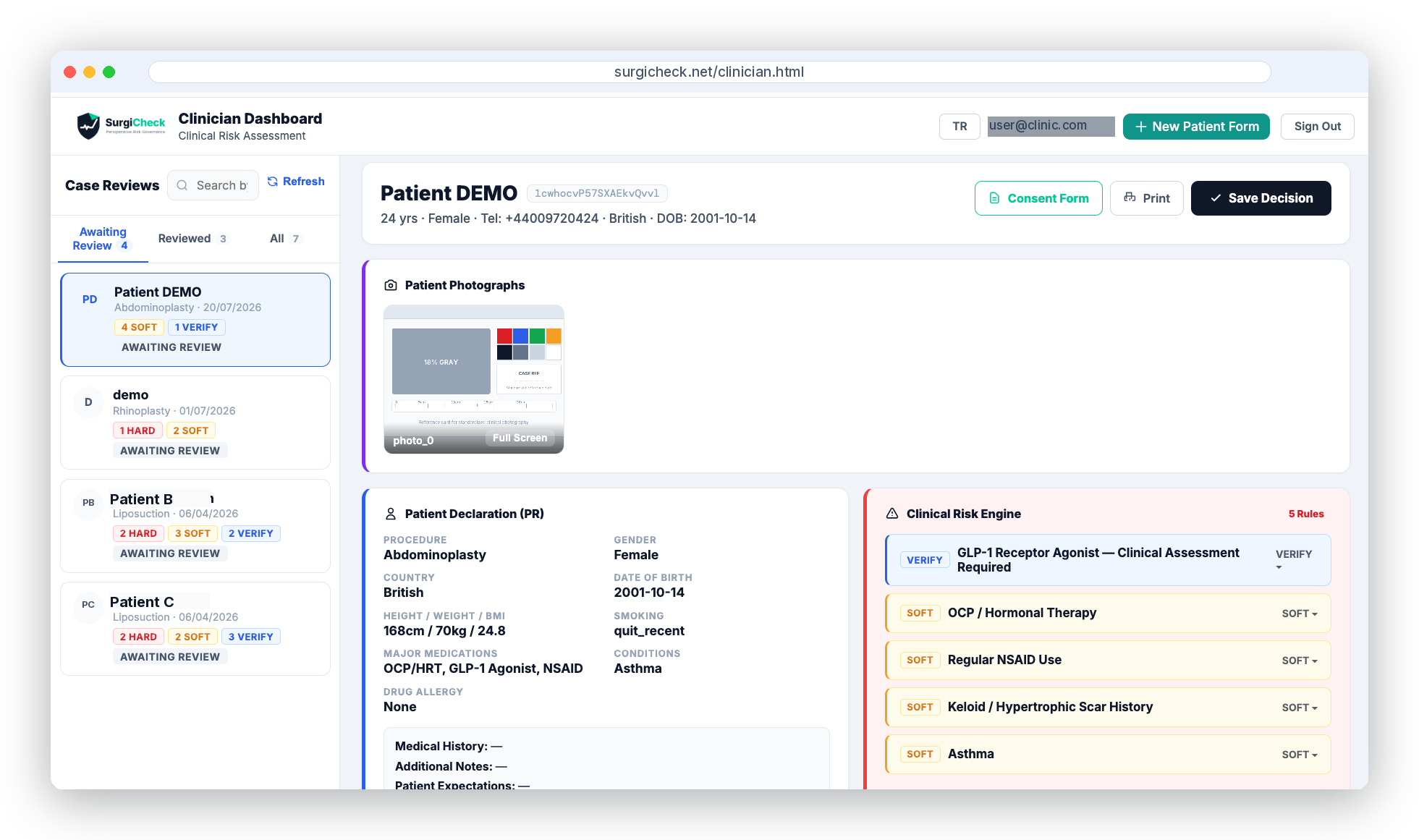
The Actual Clinician Dashboard
Live case review, patient declaration, and the clinical risk engine — exactly as your clinicians see it.
Structured pre-operative screening, Montgomery-aligned informed consent, and post-operative follow-up — in a single auditable platform for aesthetic and plastic surgery clinics.
Not a Mockup
Live case review, patient declaration, and the clinical risk engine — exactly as your clinicians see it.
In aesthetic surgery, clinical risk decisions are often undocumented, inconsistent, and — when things go wrong — difficult to substantiate.
Post-operative complaints increasingly centre on inadequate pre-operative risk disclosure. Without structured documentation, "the patient was told" is not a defence.
Clinics treating international patients may face additional contractual, consumer-protection, professional, and evidentiary expectations depending on the jurisdictions and professionals involved. Inconsistent paperwork can itself become a complaint trigger.
Regulatory inspections (CQC, accreditation bodies) require demonstrable, reproducible decision processes — not ad-hoc checklists or free-text notes.
Without a standardised rule set, the same patient profile can yield a different decision depending on who conducts the assessment that day.
Since the UK Supreme Court ruling in Montgomery v Lanarkshire Health Board (2015), clinicians are legally required to disclose all risks that a reasonable patient in that individual's circumstances would consider material — not just risks the clinician considers significant.
This creates a documentation obligation that generic consent forms cannot satisfy. Each patient's risk profile must be individually assessed and recorded.
Not a communication tool. Not a bloated EHR.
Paper consent forms and WhatsApp-based patient follow-up are not a standard — they are a liability. Large clinic management systems, on the other hand, take months to implement and are built for scale your clinic doesn't need. SurgiCheck fills the gap between the two: a lightweight risk governance engine that requires no installation, goes live in 48 hours, and helps reduce documentation gaps while supporting consistent perioperative risk governance.
Every SurgiCheck pathway — INFO, VERIFY, REVIEW, or DEFER — is linked to a defined clinical rationale, source, and required workflow action, grounded in published clinical guidance: ASA, ISAPS, ESAIC, BAPRAS, RCOG, or BSH. The system does not generate a decision — it structures the clinician's decision process and supports it with documented rationale.
When a post-operative complaint arises and a patient's solicitor asks "Why was this patient cleared for surgery?", the answer is not "the system approved it" — it is "this specific risk profile was evaluated against these published criteria, the clinician reviewed the flags, and the decision was recorded with documented rationale."
SurgiCheck does not constitute medical advice. Clinicians must exercise independent professional judgement in all cases.
Pre-operative to post-operative — documented risk management at every stage.
Standardised rule engine surfaces structured risk flags at patient intake — with full rationale and guideline references — informing the clinician's Suitable / Conditional / Not Suitable decision.
Procedure-specific consent documentation is generated from the assessed risk profile to support — not replace — the clinician-patient consent discussion. Digital signature, timestamp, and append-only, versioned Firestore archive.
Structured follow-up questionnaires at defined intervals (Day 1, 3, 7, 14, 30). Abnormal responses trigger clinician alerts automatically.
Rule set versions, decision timestamps, and the data behind every clinical outcome are recorded automatically. Append-only and versioned by design.
Role-based access architecture designed for surgeon, nurse, clinic coordinator, and medical director workflows. Production deployment requires clinic-specific role and tenant configuration.
All data in transit over TLS. Special category health data handled under GDPR Art. 9(2)(h) — lawful basis documented in privacy notice. Patient data is not sold or disclosed to third parties for advertising or unrelated commercial purposes.
Eight structured steps — seamless perioperative workflow in a single platform.
Standardised online form with procedure context, medical history, and medications.
System generates initial risk flags from patient-reported data. Case record created.
Clinician completes CV fields: ASA class, smoking status, anticoagulants, measured BMI.
Flags re-evaluated with CV data. Clinician records Suitable / Conditional / Not Suitable with mandatory rationale.
Procedure-specific consent form generated from patient's individual risk profile. Digital signature captured and archived.
System locks case record. Printable clearance report generated. Case content is locked against direct overwrite from this point; corrections are recorded as new, timestamped versions.
Structured patient follow-up at Day 1, 3, 7, 14, 30. Accessible without login.
Responses exceeding alert thresholds trigger clinician notification immediately.
SurgiCheck's rule set and documentation architecture are aligned with the regulatory frameworks relevant to clinics treating UK and European patients.
The platform's individual patient risk assessment and per-profile consent generation directly supports the clinician's duty to disclose material risks to the specific patient — not a generic checklist.
Health data is processed under the lawful basis of medical purposes. Patient data is not sold or disclosed to third parties for advertising or unrelated commercial purposes. Append-only records support data integrity obligations. Privacy notice provided at patient intake.
Clinical pathways are informed by current professional guidance and consensus sources — BAPRAS, ISAPS, ASA, ESAIC, RCOG, BSH, and ADA — with rule versions and source references recorded for clinician review.
The platform's mandatory rationale field and clinician verification steps support the GMC documentation standard: decisions must be recorded, explainable, and traceable to clinical criteria.
Case records, consent documents, and follow-up responses are preserved as an append-only audit trail — the original entry is never overwritten. Corrections are recorded as new, timestamped versions alongside the original. Rule set versions are logged at decision time — a complete, traceable, and review-ready audit trail.
A typical cross-border patient assessment — UK patient, rhinoplasty, multiple risk flags.
Risk Signals Identified
✓ All flag sources are named clinical guidelines — documented and traceable.
Personalised Risk Items (Montgomery-aligned)
Next follow-up: Day 14 — scheduled per rhinoplasty protocol. All responses logged to an append-only audit trail.
Aggregate risk signal data and decision outcomes — available to clinical directors and quality managers.
SurgiCheck provides decision support — final surgical decisions remain entirely under clinician control.
| Feature | Paper Forms / WhatsApp | SurgiCheck |
|---|---|---|
| Standardised assessment criteria | ✗ Variable | ✓ Always |
| Append-only audit trail | ✗ Manual notes | ✓ Automatic |
| Decision explainability | ✗ Implicit | ✓ Guideline-referenced |
| Triage time | 15+ min | ✓ <3 min |
| Montgomery-aligned consent | ✗ Generic form | ✓ Per risk profile |
| Post-op complication monitoring | ✗ Patient calls in | ✓ Structured protocol |
| GDPR-aligned privacy architecture | ~ Variable | ✓ Privacy-first |
Three tiers designed for every stage of clinical adoption. GBP pricing available on request.